|
|
- Home
-
Resources for Living Well with PD
- Start Here What You Need to Know about PD >
- Living Well with PD: Start Today
- PD 101 Free ebook
- Your Questions About PD Answered in our Blog
- Community Resources >
-
Articles & Research on PD
>
- BRAIN PROTIENS MARKERS FOR PARKINSONS DETECTION
- GUT MICROBIOME EARLY PREDICToR OF PD
- NEW DBS SETTINGS MAY IMPROVE SPEECH IN PD
- BRAIN PATTERNS LINKED TO LEVODOPA INDUCED DYSKINESIA
- BRAIN MODELING TO PREDICT PD PROGRESSION
- WEARABLE DEVICES FOR TRACKIN PD PROGRESSION
- BRAIN ACTIVITY PREDICTOR OF PD PROGRESSION
- DEEP BRAIN STIMULATION PD
- UNDERSTANDING GAIT IN PD
- MUSIC MAY IMPROVE GAIT IN PD
- GOLF COURSE PROXIMITY AND INCREASED RISK FOR PD
- Social Support Improves PD Symptoms
- Exercise Improves PD Outcomes
- Genetic Role in PD
- Advances in PD
- Genetic Link to PD
- Exercise and improved executive Functioning with PD
- Exercise and Fall Prevention with PD
- Intimacy and PD
- spinal cord neuroprosthesis and PD
- Advance Care Planning and PD
- Cognitive Impairment Treatment PD
- Mercury and PD
- Cognitive Remediation Therapy
- COVID Vulnerability and PD
- Postural Instability Severity PD
- Early Trial for Treatment Shows Promise
- Biomarker Found
- Therapeutic Benefits of Dance
- Ultrasound Therapy for PD
- Improvisational Theatre for PD
- PD Detection using AI and Breathing Patterns
- ALTERNATIVE MOVEMENT EXERCISE
- NON INVASIVE TREATMENT R-TMS
- Group Therapy
- Multidisciplinary Approach to PD
- VIBRATING GLOVE SHOWES PROMISE
- Prevalence of PD Underestimated
- Differences in Men and Women with PD
- Intermittent Fasting for PD
- Meditation and Complementary Therapy for PD
- Cognitive Impairment and PD
- Aerobic Exercise Alters Brain Function in PD
- A-Synuclein Biomarker
- Mediterranean Diet for PD
- Regular Exercise Improve PD Quality of Life
- Videos of PD Talks
- PD Assistive Items
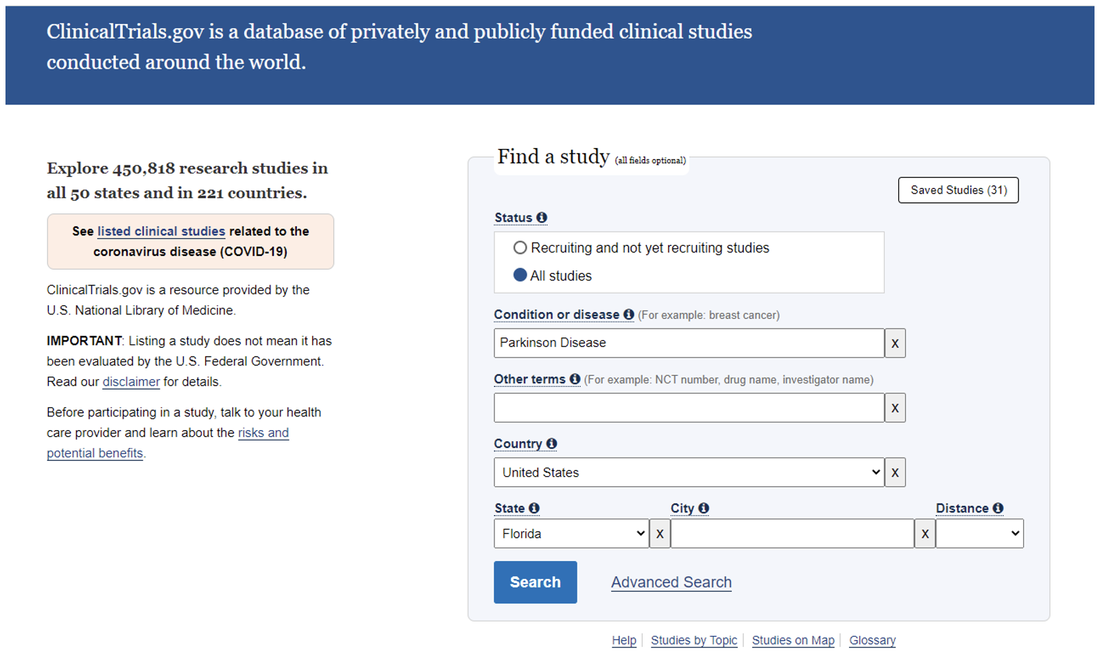
- Participate in a PD Study
- Members Only
-
Programs & Events
- About Us
- Become a Member
- CONNECT WITH US
- SUPPORTING OUR MISSION
- Home
-
Resources for Living Well with PD
- Start Here What You Need to Know about PD >
- Living Well with PD: Start Today
- PD 101 Free ebook
- Your Questions About PD Answered in our Blog
- Community Resources >
-
Articles & Research on PD
>
- BRAIN PROTIENS MARKERS FOR PARKINSONS DETECTION
- GUT MICROBIOME EARLY PREDICToR OF PD
- NEW DBS SETTINGS MAY IMPROVE SPEECH IN PD
- BRAIN PATTERNS LINKED TO LEVODOPA INDUCED DYSKINESIA
- BRAIN MODELING TO PREDICT PD PROGRESSION
- WEARABLE DEVICES FOR TRACKIN PD PROGRESSION
- BRAIN ACTIVITY PREDICTOR OF PD PROGRESSION
- DEEP BRAIN STIMULATION PD
- UNDERSTANDING GAIT IN PD
- MUSIC MAY IMPROVE GAIT IN PD
- GOLF COURSE PROXIMITY AND INCREASED RISK FOR PD
- Social Support Improves PD Symptoms
- Exercise Improves PD Outcomes
- Genetic Role in PD
- Advances in PD
- Genetic Link to PD
- Exercise and improved executive Functioning with PD
- Exercise and Fall Prevention with PD
- Intimacy and PD
- spinal cord neuroprosthesis and PD
- Advance Care Planning and PD
- Cognitive Impairment Treatment PD
- Mercury and PD
- Cognitive Remediation Therapy
- COVID Vulnerability and PD
- Postural Instability Severity PD
- Early Trial for Treatment Shows Promise
- Biomarker Found
- Therapeutic Benefits of Dance
- Ultrasound Therapy for PD
- Improvisational Theatre for PD
- PD Detection using AI and Breathing Patterns
- ALTERNATIVE MOVEMENT EXERCISE
- NON INVASIVE TREATMENT R-TMS
- Group Therapy
- Multidisciplinary Approach to PD
- VIBRATING GLOVE SHOWES PROMISE
- Prevalence of PD Underestimated
- Differences in Men and Women with PD
- Intermittent Fasting for PD
- Meditation and Complementary Therapy for PD
- Cognitive Impairment and PD
- Aerobic Exercise Alters Brain Function in PD
- A-Synuclein Biomarker
- Mediterranean Diet for PD
- Regular Exercise Improve PD Quality of Life
- Videos of PD Talks
- PD Assistive Items
- Participate in a PD Study
- Members Only
-
Programs & Events
- About Us
- Become a Member
- CONNECT WITH US
- SUPPORTING OUR MISSION